
Multiple Myeloma
Multiple myeloma is a rare bone marrow cancer that occurs mostly in the elderly. Multiple myeloma accounts for 1% of all cancers and 10% of hematological cancers. Its incidence is around four in 100 thousand. On average, around three thousand multiple myeloma diagnoses are made annually in Turkey.

When B-lymphocytes, one of the main defense cells of our immune system, encounter microorganisms, they turn into plasma cells and produce substances we call antibodies (immunoglobulin, Ig). Multiple myeloma is a disease of blood cells that secrete proteins such as IgG, IgA, or light chain, called M proteins. However, in multiple myeloma, plasma cells proliferate uncontrollably and produce excessive amounts of one type of immunoglobulin. However, dangerously low levels of other immunoglobulin types occur and patients become susceptible to infections.
In addition to this picture, these rapidly multiplying cells (cancer cells) accumulate in the bones and bone marrow and form masses that destroy bone tissue. Over time, these tumor masses cause bones to weaken or break and the body’s resistance to infections to decrease. The emergence of myeloma, which is generally seen in people over the age of 60, is caused by chemicals, antigens and infections that are exposed throughout life. Myeloma, which is an adult disease, is never seen in children.
Multiple myeloma differential diagnostic tests should be performed on anyone over the age of 40 who consults a physician with complaints of waist, back pain and/or kidney failure or fatigue.
What are the symptoms of Multiple Myeloma?
The majority of multiple myeloma patients consult a physician with unexplained back or bone pain, fatigue, and lung infections. Generally, unexplained bone pain and/or pathological fractures (the presenting complaint of 26-34% of patients) over the age of 60 are important clues that should suggest this disease. Patients most often consult physical therapy, orthopedics, sometimes internal medicine and general practitioners due to their pain. Since most of them are elderly people, they are usually diagnosed with arthritis and given painkillers for treatment. While these painkillers reduce the severity of pain to some extent, they may also cause kidney disorders or increase existing diseases.
Complaints related to high calcium levels such as fatigue, nausea, drowsiness and drinking plenty of water are common in patients. While some of the patients may apply to nephrology units with complaints of kidney failure, some may apply to physical therapy or orthopedics departments with back pain, and some may apply to internal medicine and/or hematology specialists with complaints of fatigue, fatigue and pallor due to anemia. Depending on the deficiency in the immune system, the other reason why these patients consult a physician may be febrile illnesses (often lung and urinary tract infections).
Symptoms and Incidence (%)
Bone pain (especially back pain) – 58%
Fatigue (typically caused by anemia) – 32%
Pathological fractures – 26-34%
Weight loss – 24%
Paresthesias – 5%
Fever – 0.7%
Asymptomatic – 34%
Although myeloma is more common after the age of 60, it is also frequently seen in people between the ages of 40 and 60 in our country. However, it is rarely seen under the age of 40. Although the disease is common in some families, there is no genetic predisposition among its causes.
What causes Multiple Myeloma?
Today, the causes that lead to multiple myeloma have not yet been fully revealed. Factors currently commonly held responsible include exposure to oil, chemicals and radiotherapy.
Although MM has not been found to be directly related to diet in studies conducted to date, it has been observed more frequently in people who consume too much animal fat and are obese. On the other hand, it is suggested that it is less common in those who consume more vegetables and fish and those who take additional vitamin C.
Occupational or environmental factors:
- Occupational exposures (relationships weak or unproven for most of the following, except in the nuclear industry):
- nuclear industry
- metal sheet industry
- Farming (pesticides – especially DDT – and fertilizers)
- wood dust
- leather tanning industry
- Other possible risk factors:
- Formaldehyde,
- Benzene,
- Hair dye,
- Spray paint,
- Exposure to asbestos.
How is the diagnosis made?
Approximately 10% of patients are detected by chance. Most of these patients are referred to a hematologist by determining the sedimentation level. However, there may be a delay in applying to a hematologist for those with kidney failure and lung infections.
Especially patients with kidney failure come to the doctor after becoming dependent on dialysis. If the diagnosis can be made early in these patients, they can be treated without being dependent on dialysis.
The diagnosis of multiple myeloma is not made with a single examination method. To make the initial diagnosis of the disease, the patient’s sedimentation, total protein, albumin values as well as the blood levels of immunoglobulins (IgG, IgA, IgM) secreted by plasma cells are examined by protein electrophoresis. Immunoglobulins may also increase due to different reasons. The important thing is to determine whether this increase is due to myeloma. It is possible to distinguish this by serum and or urine protein electrophoresis. A uniform increase in immunoglobulins in the test indicates myeloma. If the suspicion of MM persists according to the test results, then a bone marrow biopsy is performed as a further examination.
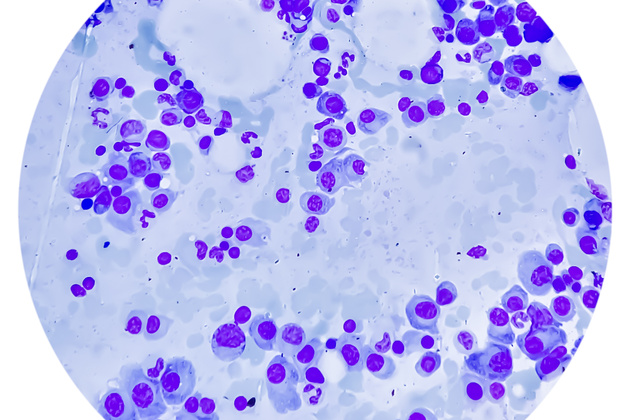
In bone marrow aspiration, the amount of plasma cells in the bone marrow is checked. Since the main site of the disease is the bone marrow, the number of plasma cells in the bone marrow increases. While the number of plasma cells is normally 1 – 2%, this rate exceeds 10% in multiple myeloma disease.
Another diagnostic method is to examine lytic lesions in bones. These are detected in radiological bone scans as images as if they were punctured with a stapler.
In this regard, the most important diagnostic criteria are the increase in plasma cells in the bone marrow, the level of immunoglobulins and lytic lesions in the bones.
Another symptom seen in these patients is the deterioration in kidney functions. Proteins secreted by myeloma cells disrupt kidney functions. Since it disrupts kidney functions, patients’ urea increases. These patients are considered kidney patients and also receive dialysis treatment.
If the organ functions of patients under 65 years of age are adequate, autologous transplantation after M-protein reduction with chemotherapy is the standard treatment.
What are the stages of the disease?
In these patients, we obtain clues about the stage of the disease and its course by looking at the presence of anemia, whether the calcium level in the blood is high, the prevalence of lytic lesions in the bones, the high level of immunoglobulin, CRP, albumin and LDH levels. The disease consists of three stages. In the past, it was predicted that those in the early stage could live for 10 years, those in the intermediate stage could live for 2 – 10 years, and those in the advanced stage could live for two years; Today, 30% of patients can be given a 10-year life expectancy.
Disease staging in general terms:
Stage – I: A small amount of cancer cells have spread throughout the body and the patient may not have any complaints.
Stage – II: spread in the body is greater than the first stage.
Stage – III: large numbers of cancer cells have spread throughout the body. At the same time, there is anemia, an increase in the amount of blood calcium due to the destruction of bone cells, more than three tumors in the bone or M-protein in the blood; M-protein is a protein that is considered a specific marker in this disease.
Disease staging is an important step that greatly helps determine clinical treatment. In the light of the information collected at this stage, each physician tries to choose the most useful and appropriate treatment scheme for his patient.
How is it treated?
Treatment options should be determined according to each patient’s clinical condition, taking into account the patient’s general condition, complaints and stage of the disease. For this reason, patients who do not have any symptoms and/or complaints are followed up with general condition and disease status evaluations, while those who have complaints and are diagnosed with a progressive disease are first treated with medication (chemotherapy). Chemotherapy provides complete recovery in 10-50% of patients and partial clinical improvement in 50-70% of patients.
Autologous (own tissue) transplantation is applied as standard treatment for patients younger than 65 years of age and without organ dysfunction. Before stem cell transplantation, the patient is given chemotherapy to minimize the disease. Then autologous stem cell transplantation is performed. The probability of loss of life in autologous transplantation is less than 3%. If the patient is over 65 years of age or if autologous transplantation cannot be performed because the patient has impaired organ functions, triple or double combination chemotherapy is applied. If heart or lung functions are impaired, the patient may lose the chance for autologous transplantation. Impaired kidney function does not constitute an obstacle for autologous transplantation. However, if the patient has become dependent on dialysis, autologous transplantation is not recommended.
In parallel with the developments in technology in the last few years, drugs that can directly kill myeloma cells without damaging healthy cells have begun to be used in elderly patients and patients who cannot undergo autologous bone marrow transplantation.
In addition to all the treatment options mentioned above, adjunctive treatment methods also have a place in the treatment of multiple myeloma. Radiation therapy may be given to bones where bone pain is intense and/or at high risk of fracture to relieve pain and prevent complications. Oral medications are also used to prevent complications due to deterioration of bone architecture. If a pathological fracture develops despite all efforts, the fracture is immediately treated with surgery.
As mentioned before, additional problems such as anemia and febrile illness due to impaired immune system, which affect the general condition and quality of life of patients, can be overcome with supportive treatment. For anemia, erythrocyte transfusion or administration of substances that stimulate the production of red blood cells (erythropoietin) and, when necessary, appropriate antibiotic treatment constitute an important part of the supportive treatment options.
Is it possible to be protected?
Today, since the risk factors that cause multiple myeloma have not yet been fully revealed, it can be said that trying to stay away from environmental factors and occupational risk factors, maintaining a healthy and balanced diet and regular health checks may be valid methods for protection.
Is it possible to make an early diagnosis?
Especially people over the age of 50 should be advised to consult a physician immediately if they have frequent infections, complain of bone pain, frequent nosebleeds, long-term bleeding from a small cut, easy bruising, and abnormal fatigue.
Regular health check-ups are of great importance in early diagnosis.